
The short answer lies in a very old quote:
“The dose makes the poison.” –Paracelsus
Like most of you, I have been taught to believe that fluoridated water is one of the greatest interventions of the last century. Believing what I learned in dental school, I have not had much interest in reviewing the history of water fluoridation and any possible safety issues with this public health practice. But as I have been studying nutrition and the airway, a natural topic to include in the basic necessities of life (air, water and food) would be to look at what’s in our water.
In honor of brevity, I am going to highlight my top three concerns (don’t worry, I have MANY more) that I have with continuing the practice of adding fluoride to our public water systems: the source, the inability to control dosage and the lack of sufficient study regarding long term effects. For the past two years I have been researching the topic of water fluoridation and it’s taken me this long to figure out how to present a potentially controversial topic in a way that helps to bring some clarity. If you don’t wish to read further, I can summarize my research by saying that most of us likely won’t be harmed by the small amount of fluoride added to our water but I expressly have concern over the lack of choice in the matter for the majority of American citizens.
First and probably the most concerning discovery is what is used to fluoridate public water systems. My assumption had been that pharmaceutical grade NaF (sodium fluoride–what is in most over the counter toothpastes) was used as the source. But sadly this is not the case and 90% of the US water systems are fluoridated using the toxic chemical waste from the wet-scrubbing systems of the phosphate industry. If the US government did not purchase this toxic waste to dilute into our water as a source of fluoridation, the corporations would be left with the onerous financial burden of properly disposing of the hexafluorosilicic acid. Once the toxic soup is purchased by the government, it is considered a product and no longer is under the jurisdiction of the EPA. Most notable is that international law prevents the dumping of this material into oceans and waterways but when diluted it is acceptable in our water for drinking.
Most citizens, whether in the medical field or not, recognize that pharmaceutical interventions have a dosing recommendation based often on age and/or weight. Very little in this world is good in a ‘one size fits all’ dosing. The level of fluoride in our drinking water is targeted to a range of 0.7-1.0ppm (parts per million). Early studies (albeit not randomized or blinded) established this level of 1.0ppm (dosing was later reduced to 0.7mm in the early 2000s) as the benefit for reducing tooth decay while only a small portion of the population would potentially be harmed by unsightly dental fluorosis. Dental fluorosis is the undesirable brownish and sometimes white mottling of tooth structure due to an overexposure to fluoride. The amount of water consumed daily can vary vastly: some take in far less than 1 liter per day while serious athletes and those with strenuous jobs may consume 2-3 times this much water in a 24 hour period. Infants who are bottle fed have the highest exposure by bodyweight in the population because of their sole reliance on liquids for their daily caloric needs. Also those with kidney dysfunction are likely to be more susceptible to overexposure due to their bodies’ decreased ability to filter toxins.
Since the introduction of fluoride into municipal water systems, no robust long term studies have been done to understand the vast implications this measure could have on humans, animals and our environment. Less than 1% of the water that is fluoridated actually is consumed by humans, 99% is for external use like bathing, washing dishes, watering our lawns etc. There have been small studies often with animal subjects that demonstrate possible harm to the pineal gland, the kidneys, the thyroid gland, the bones, the joints and the reproductive system. Being heard in court at the end of this month are the findings from a multi-year review of current research (meta-analysis) that finds an association between fluoride exposure and lowered IQ. The National Toxicology Program (the government agency responsible for the literature review) has concluded that fluoride is presumed to be a cognitive neurodevelopmental hazard to humans. The court hearing will be to what extent the level at which we currently fluoridate poses this risk and should we as a nation continue this practice knowing that some may be harmed.
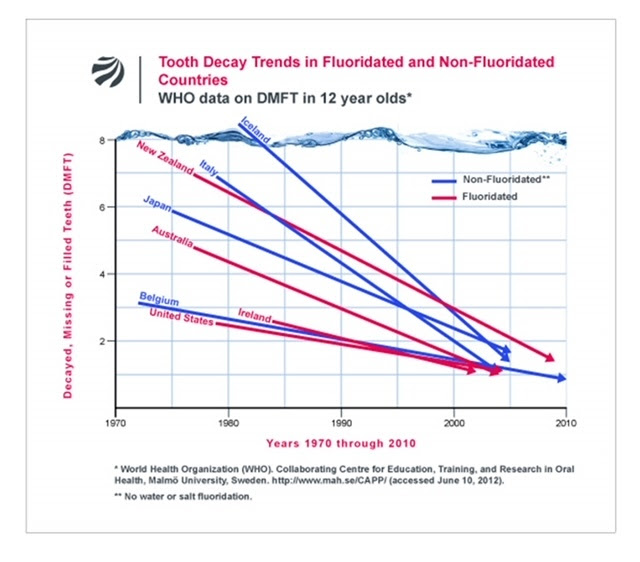
In closing, this has been a heavy topic for me. I started my research firmly in the camp that water fluoridation has profoundly changed the course of my profession by decreasing the incidence of tooth decay. This is what I had been taught and until I did my own investigation and research did I become painfully aware of facts that my profession has tried very hard to hide. My intention of presenting this information is to bring awareness and to highlight that most of the developed world does NOT fluoridate their water. Around the same time we began to fluoridate, toothpaste with fluoride became widely available and oral hygiene instruction became common practice at dental offices. Countries that do not fluoridate saw a similar decrease in decay rates (see graph) likely due to these interventions.
There is so much more I could share and based on interest level, I may go into more detail in a future newsletter. As always, it is an extreme honor to be entrusted with your care. My staff and I view each of you as part of our family and we do not take lightly the responsibility of providing your dental treatment.
Respectfully,
Jessica
